Folded-Flap Palatoplasty: the better way to improve brachycephalics.
Brachycephalic breeds such as bull dogs, pugs, and boston terriers shared the anatomical variation of short noses and all of the consequences that go with the condition. Varying degrees exist and some dogs lead relatively normal lives, however, a vast majority have moderate to severe respiratory limitations which may be significantly improved with palate modifying surgery. Classically this was simply shortening the palate. The folded-flap palatoplasty takes this to the next level and not only shortens the palate, but allow decreases the thickness.

photo credit: www.poshchicago.com
Bull dogs, French bull dogs, Boston Terriers, Pugs and combinations there of are loved by many due to their short-nosed look. Unfortunately with this look comes other anatomical shortcomings including elongated soft palate, hypoplastic trachea, stenotic nares, aberrant ethmoid turbinates, and everted saccules. Palates, nares and even turbinates can be modified surgically. The classic palate repair involved shortening of the palate with sharp excision via scissors or a blade, laser or vessel sealing devices. Simply shortening the palate is highly effective; however significant stridor is still noted in some dogs.
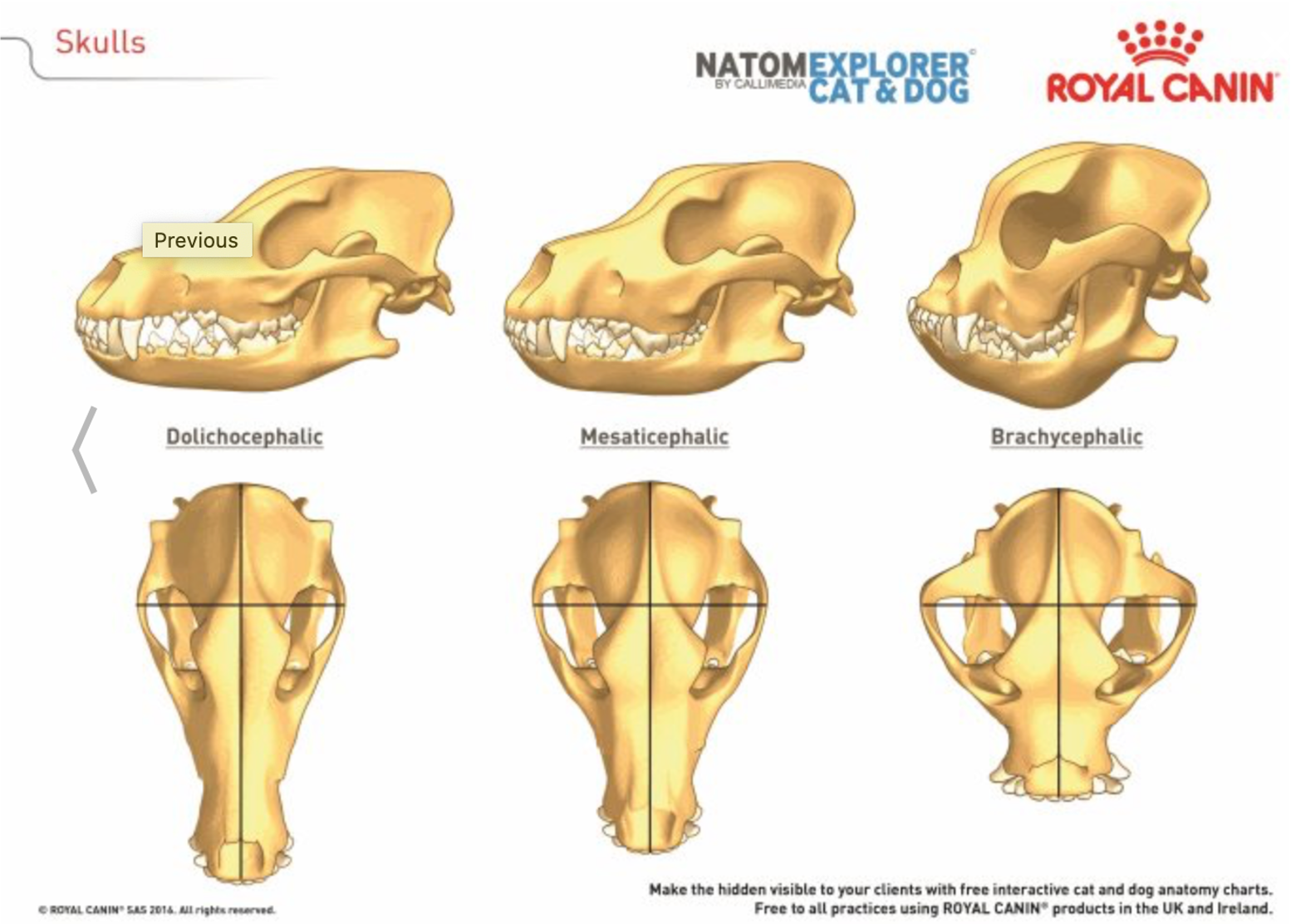
The brachycephalic skull is modified in cranial and caudal aspects, literally shortened in dimension. The tongue, palate, turbinates and other soft tissues remain of relatively normal size, struggling for room in the short but wide enclosure. (credits royalcanin.com)
elongated palate
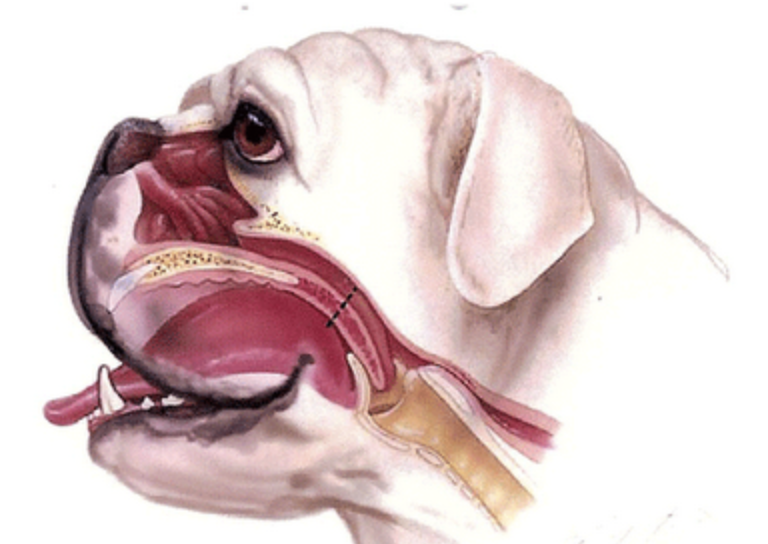
This lateral view and partial cross section emphasize the elongated soft palate, which partially obstructs the airway. The turbinates obstruct the nasopharyngeal airflow. (veazievets.com). Image below shows this in further detail.
The traditional palate surgery shortens the elongated palate. Initially, there was concern of not overdoing the procedure and taking more palate later, if necessary. There after, modified procedures evolved taking more palate without consequence.

The blue line denotes the traditional staphylectomy cut site. The traditional landmarks are incision of the palate at the level of the caudal tonsils. The red line denotes the modified staphylectomy site. The modified incision allows for removal of more palate thus opening up the airway significantly more than previous. (images courtesy of VetRecord)

Image courtesy of Cambridge University
Once the appreciation of not only an elongated but thickened palate was appreciated, new surgical perspectives were developed to improve the outcomes of palate modification. In 2008, Drs. Findji and Dupre published a technique in which the palate length was both shortened and thinned (Vet. Med. Austria / Wien. Tierärztl. Mschr.* 95 (2008), 56 - 63). A clear pictorial article was published in 2013 in Clinician’s Brief.

Image: Clinician’s Brief 2013 Findji and Dupre
Using the technique of Findji and Dupre, the caudal aspect of the palate is tractioned cranially with the use of stay sutures. A trapezoid of tissue to be removed is outline with electrocautery.
The majority of soft tissues are removed between the nasopharyngeal and oropharyngeal mucosae, including ventral mucosa, connective tissue, part of the palatines and elevator palatine levi muscles. The remain preserves the inner most layer of nasopharyngeal mucosal tissue. The caudal aspect is then advanced rostrally and flapped in place. The provides a shorter, thinner palate with the added benefit of a more rostral incision, out of the immediate airway. The more rostral incision helps with breathing and inflammation post operatively.

Tractioning of the caudal mucosa in a rostral direction is depicted here.

The tissue to be excised is demarcated with electrocautery (pin point tip). The shape is generally trapezoidal.
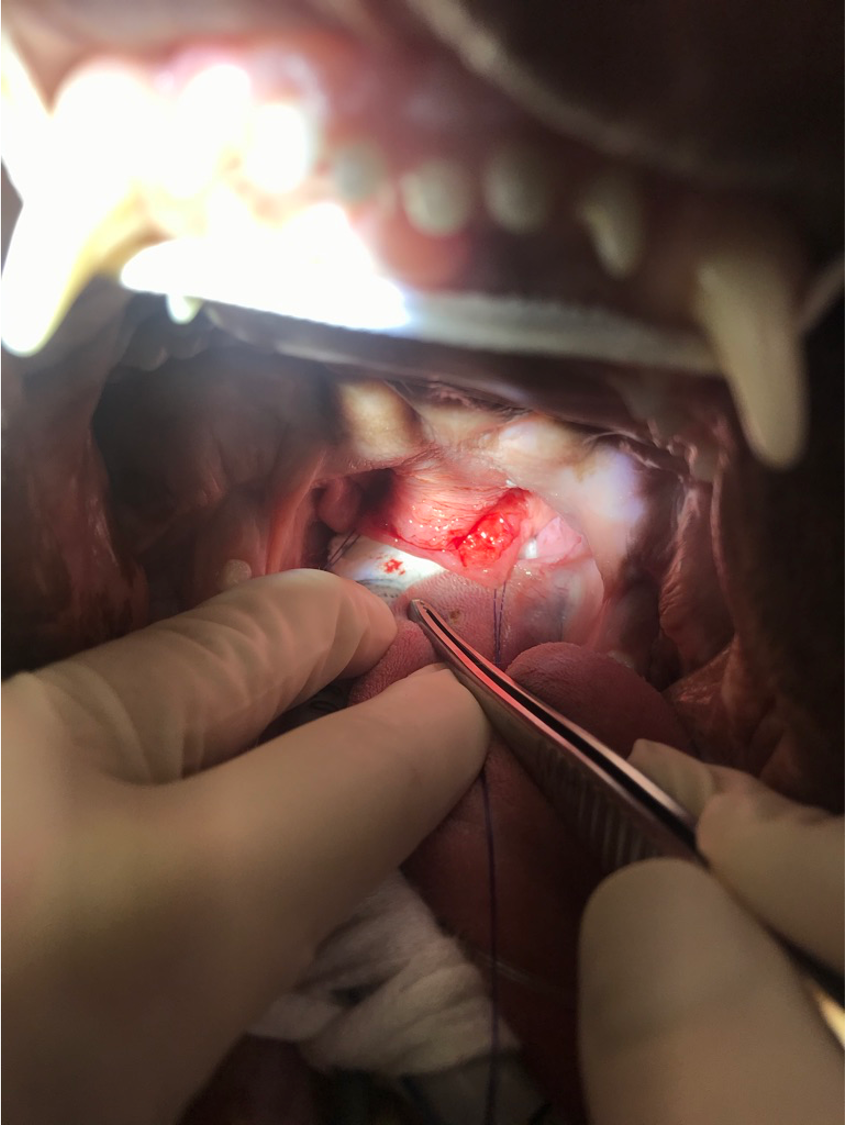
The view displays the beginning of partial thickness excision of soft tissues. Excision is meticulous, ideally cauterizing vessels prior to bleeding to improve visualization. Largest vessels are dorsal lateral (in tissue not yet excised in this photo).

In this picture, all of the tissue is excised. Stay sutures remain and next tissue will be advanced rostrally and secured.

Yellow arrows indicate the direction of advancement. The caudal most tissue where stay sutures are will excised just prior to closure.

This picture displays the final product of the FFP procedure. The sutures may be placed as interrupted or continuous (as selected here). By the procedure’s end the nasopharyngeal ostium should be visible.

At the conclusion of the FFP, the everted saccules may be removed, however, I choose to leave them in most cases as I do not like the added inflammation and hemorrhage and theoretically they should resolve with decreasing airway turbulence. The nares may be addressed at this point as well. While doing the nares, a mannitol-soaked gauze may be placed between the endotracheal tube and the palate. This is removed prior to extubation. (personal communication with Dr. Bryden Stanley)

Wedge resection of the nares can be completed in the central portion or laterally. The wedge is created with an 11 blade. I place a cotton-tipped applicator in the nares opening to attempt to stop hemorrhage from draining into the nasopharyngeal region. The wedge is closed with absorbable or non-absorbable suture. If a patient is difficult to restrain, I will use an absorbable suture such as 4.0 monocryl, to avoid removal.

The image on the left in a French bull dog prior to nares resection. Note the pinched nares. The picture on the right is immediately post operative after the nares were resected (lateral). Note how the nares are opened up.